
The Covid-19 pandemic has put the medical device industry under intense pressure to supply huge amounts of equipment, with the most urgent challenge to plug the gap in the number of medical ventilators required.
Analytics company GlobalData estimates about 880,000 ventilators will be needed worldwide to meet the demand caused by Covid-19, with data suggesting one in six people who contract the disease will become seriously ill and need hospital treatment.
In the most severe cases, the virus damages the lungs, making it harder to breathe and causing the body’s oxygen level to drop — when this happens, patients will often be put onto a medical ventilator to manage the problem.
To help plug the ventilator gap, governments are turning to non-medical manufacturers — including those in the auto and technology sectors — to develop devices.
One of the main reasons why there’s a global shortage of the devices is because large-scale ventilator manufacturing hasn’t traditionally been big business.
Most machines last between 10 to 15 years, meaning there’s never any urgent from customers under usual circumstances. This is coupled with the device’s basic functionality not drastically changing for more than 60 years.
History of the ventilator
The history of the medical ventilator dates back nearly 100 years to the late 1920s, when the drinker respirator was developed.
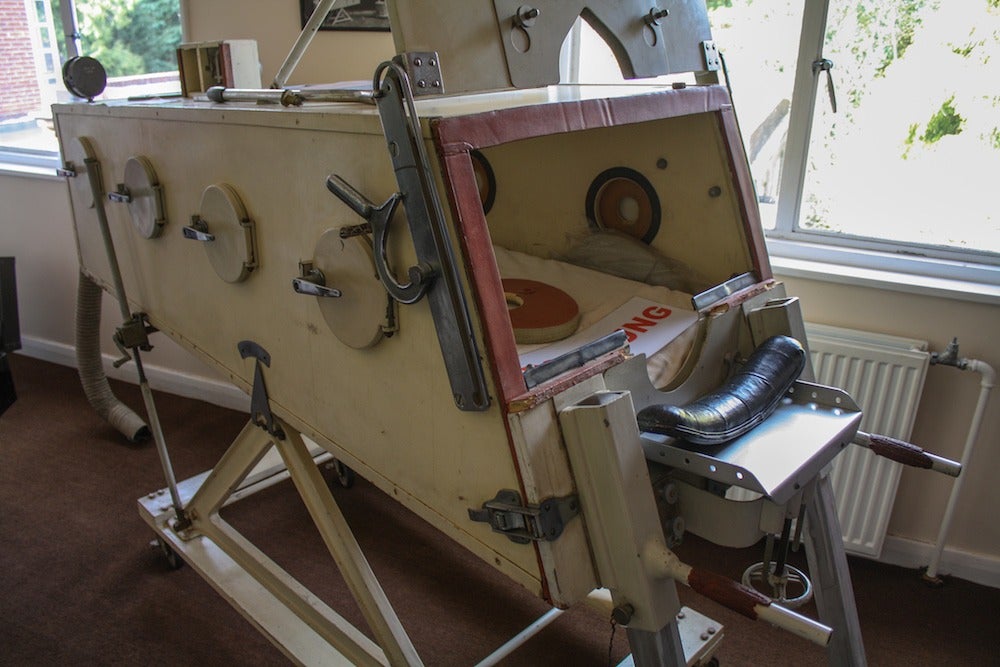
Known as the “iron lung”, this device was used between the 1930s and 1950s to help polio victims to breathe.
It achieved this by using negative air pressure to help patients breathe while lying inside a sealed chamber.
The next innovation in ventilator technology was based on a system used to supply oxygen to fighter pilots flying at high altitude during the Second World War.
This technology was implemented during the 1950s, with the ventilators using positive pressure to pump air into the lungs through a face mask or a tube inserted in the throat.
This evolved over the decades, with a greater focus placed on oxygenation failure — which led to the identification of the acute respiratory distress syndrome (ARDS).
Over more than 60 years since, many technical aspects of ventilators have dramatically improved, including flow delivery and exhalation valves.
What’s required to build a ventilator?
To help guide businesses new to manufacturing ventilators, the UK government’s regulator the Medicines and Healthcare products Regulatory Agency (MHRA) published details outlining what the devices must be able to do.
The proposal, set out by the organisation in mid-March, stated the devices would be required to perform short-term stabilisation for a few hours.
This must be possible to extend up to a day for patients in the worst condition as the bare minimum function.
Devices must also have a continuous mandatory ventilation mode (CMV) — which allows for breaths to be set at a minimum rate.
This should be regulated through a pressure-controlled ventilation system — allowing the patient to breathe in, with the volume achieved measured and displayed.
Alongside this, ventilators should have a spontaneous breathing pressure support mode for people breathing to some extent themselves.
The rules set out by the MHRA also outline infection control guidelines for ventilator equipment.
It states that all of the parts coming into contact with the patient’s breathing must be either disposable or designed to be reusable.

Alongside this, all external surfaces must be able to be cleaned manually by healthcare workers.
The ventilators must be fitted with alarms triggered if there is a gas or electricity supply failure, and in the event of problems with oxygen pressure going to the patient.
Any monitoring carried out by the device — including measuring a patient’s current airway pressure — must be displayed continuously so a doctor or nurse using it can verify the information.
To be approved for use, the ventilators must be reliable and capable of continuous 100% operation for at least 14 days.
Alongside this, it has to be intuitive to use for qualified medical personnel, requiring no more than 30 minutes’ training for a doctor or nurse with some ventilator experience.
Instructions for use should also be built into the devices’ labelling, including clear labelling of all critical functions.
When it comes to testing the final devices — the UK’s MHRA accepts that a full demonstration is unrealistic in the time frame required, however, compliance must be proven to ensure patient safety.
For example, usability testing at both the prototype and final production stages of the ventilator is required.
This involves someone operating the devices wearing complex protective clothing such as goggles, a face shield, two layers of gloves and a surgical gown.
How did a company from outside the medical device industry design and build a ventilator?
When the UK government initially asked for more ventilators, it spoke to a wide variety of manufacturers to see if they could help.
One of these businesses was vacuum developer Gtech.
Recalling the initial conversation with a government representative on a Sunday morning in mid-March, the company’s founder and owner Nick Grey says: “I told him ‘I don’t know what a ventilator is really, but I’ll have a little look’, so he sent me over a couple of web links.
“And later that day, I was invited into an online call with around 20 or 30 people to discuss the proposals.”
The firm aimed to design a device that was fairly simplistic and easy to produce.
The first area Gtech looked into was how they were going to make the pneumatic cylinder — which is used to push air to the patient — for the device, however, it found a lot of materials weren’t suitable for use with oxygen.
Grey adds “I tasked the guys with making a pneumatic cylinder that could work with oxygen out of raw materials.”

The designers discovered the best material to use was a repurposed hospital syringe, which is a long tube with a plunger.
Grey says: “You stick a pipe on the end and when you blow it up, it’ll expand and when you let the air out, it’ll contract’.
“We then made a two-port valve from brass and stainless steel, no seals or anything so it was very safe with oxygen and very simple to make.
“But it stalled at the end of its stroke, so the minute the valve cracked, it would just reach an equilibrium and it wouldn’t reciprocate.”
To counteract this problem, the team developed a spring throw-over mechanism — which meant when the piston got to a certain point before the end of the stroke, the spring would be compressed.
This meant it oversent — going over the valve instantly, and moving back the other way.
Grey says: “So it was very simplistic and reliable.
“We also put some valves in to control the inspiration and expiration — that’s the breath-in and the breath-out that the hospital controls — and it worked beautifully.”
Although Gtech was turned down as a ventilator supplier in the UK, the company is offering its design to countries around the world.




